What is a dacryocystorhinostomy (DCR)?
A DCR is a type of surgery that is used to treat blocked tear ducts in adults. It creates a new passageway between the tear duct sac and the nose, bypassing the blockage and allowing tears to drain normally again. The operation usually takes about one hour.
The operation is normally performed under local anesthetic (numbing the area to be operated) with sedation, although occasionally if requested you may be asleep (general anaesthetic). This will be discussed with you.
The two main types of procedures are:
- External DCR – Is the most common operation for blocked tear ducts and has a success rate of over 90%. A small incision is made on the side of the nose to gain access to the tear sac. A small amount of bone between the tear sac and the nose is removed. A new passage is made for the tears to go down and some flexible tubes are placed in the new passage to keep it open. The tubes are usually removed after 6 – 8 weeks in the clinic. The stitches on the side of the nose will be removed after approximately one week.
- Endoscopic DCR – Uses a telescope to look up the nose and locate the site of the blockage, which is then opened up surgically.
*Mr Kamalarajah does not perform endoscopic DCRs*
What happens before the operation?
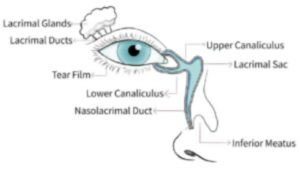
Normally, the tears that wash over the eye drain away through a system that runs from the corner of the eye to the inside of the nose. If there is a blockage in this system the eye can start watering and you may be more prone to infections.
To unblock the area, warm compresses and massage may be tried first.
The blocked tear duct is diagnosed in clinic by probing it. This is called syringing and involves flushing salty water down the tear duct. If the tear duct is open then you will taste the salty water in your throat.
Once you and your surgeon have agreed that you should have a DCR operation then your name will be placed on the waiting list for the procedure.
How do I prepare for the operation?
Medication
We need to know what tablets and medicines you are currently taking and also if you are hypersensitive to any substances. At the pre-operative assessment in clinic you will be advised on what pre-operative preparations you need to make such as altering medications.
If you are on warfarin or aspirin tablets it is important that you inform your surgeon, as these can lead to bleeding during or after the operation. You may need to stop your aspirin 10 days before surgery but the need to stop your warfarin will be discussed with you at pre-operative assessment.
Admission to hospital
You will generally be admitted to hospital on the day of your surgery, although in some circumstances you may need to be admitted the day before. This will be discussed with you.
What are the complications or risks of a DCR?
- You can expect slight swelling and bruising of the eyelids, which usually resolves in a fortnight.
- There is a small risk of infection with any surgery, but this rarely happens after a DCR.
- It is normal to have slight bleeding from your nose after surgery; this usually settles in a few days.
- A severe nosebleed is a rare event which can happen up to ten days after the operation. This is more likely to happen in patients with infection, uncontrolled high blood pressure or those on blood thinning agents (e.g. aspirin, clopidogrel, warfarin, apixaban or rivaroxaban). We may ask you to stop your blood-thinning pills before surgery. However, you should consult your GP and/or cardiologist before stopping your medication, to confirm that it is safe to do so.
- The surgery can fail in a minority of patients, usually because scar tissue forms inside the nose and blocks the bypass channel. This may require further surgery to revise the bypass channel, or even insertion of a small pyrex tube known as a Lester Jones tube to bypass the entire tear duct system.
- The scar on the side of your nose usually fades and only 3% of patients notice it after three months.
- Rarely, the stent may irritate or “cheese-wire” towards the inner corner of the eye.
- The loop of the stent can occasionally protrude outwards in the inner corner of the eye where it passes from one eyelid to the other. If this happens do not tug on it but seek attention because the stent might need to be repositioned.
- The fine silicone stent may protrude from the nostril if it is cut too long inside the nose. If this happens do not tug on it but seek attention because it may need to be trimmed.
- The stent may break and spontaneously work its way out of your nostril. Do not panic if this happens and there is no need to seek attention if it comes out completely.
- Rarely, a small skull fracture can occur during the operation resulting in a leak of fluid from the brain. This can sometimes result in a meningitis. The risk of this is less than 1 in 1000 cases.
What happens afterwards?
Immediately after the operation there may be a little discomfort, some spots of blood from the nose and some facial bruising at the site of the operation, (which would be expected to resolve within 2 – 4 weeks). Occasionally, a pressure bandage will be placed over the site of the operation to reduce the bruising. This is usually removed the day after surgery. Usually you can go home on the day surgery, sometimes you may be required to stay in hospital overnight.
After care
In order to prevent infection you will be prescribed eye drops or ointment for two weeks and possibly antibiotic tablets to take for 5 – 7 days.
The first clinic appointment is 7 – 10 days after surgery to remove the stitches if they have been used. The second appointment will be 6 – 8 weeks after surgery to remove the tubes in the outpatient department. A final check is usually made six months after surgery when you will be discharged if all is well.
If you do develop bleeding from the nose that will not stop, do not dab the nose but hold the end of the nose tightly. If bleeding carries on then attend your nearest casualty department immediately, also contact the Eye Clinic to let us know that you are having a problem.
Is there anything that I should avoid after the operation?
Important points to follow
Please remember the following points:
- During the first week after surgery you may get a little bleeding from your nose. In order to minimise this, you are advised to sit up rather than lie down and to sleep with extra pillows at night. You must not blow or pick your nose for two weeks after your operation. After that you are encouraged to blow your nose to clear the blood clots. If you need to sneeze, you are advised to do this with your mouth open.
- For discomfort use pain relief medication that you would normally take for a headache.
- Also avoid exercise especially swimming for two weeks after surgery.
- Air travel is not advisable for at least seven days after surgery.
- Do not wear make up for two weeks after surgery.
- Avoid homeopathic medicines that promote fast healing.